
A Home Finger-Prick test promises to catch the hidden cardiac risks in young adults if combined with practical guidance and smarter support systems.
Study: Intentionality of Self-Educated Dried Blood Collection for Analysis of Cardiomatomal Profile in a population sample of young adults. Credit Picture: Antoniodiaz / Shutterstock
In a recent study published in the magazine PLOS ONEResearchers at Deakin University in Australia examined the feasibility of self-propelled dried blood collection (DBS) for a heart-wide profile in young adults.
Poor cardiovascular health strongly predicts cardiovascular disease. Non -contagious diseases (NCDs) is the leading cause of death in high -income countries, including Australia. Early detection of poor cardiovascular health can help reduce the weight of deaths by NCD. Young adulthood is often characterized by high -risk behaviors that adversely affect cardiovascular health.
DBS collection kits are increasingly used for remote health control. This method can reduce staff, shipping and storage costs, while improving ease, approach and accessibility. Tests have been developed for various analysts in DBS samples, including cardiac meters. However, no study examined the feasibility of the DBS collection for a heart -wide profile in young adults.
For the study
In the present study, the researchers determined the feasibility of the self-grated DBS collection for a heart-wide profile in young adults. The Mymeals study recruited the participants between April 21 and November 21, 2022, to understand heart -wide health and food choices in young adults. The participants were residents of Australia aged 18-30, who were not pregnant, nursing or in a vegetarian or Vegan diet.
Participants were mailed a DBS collection kit and instructed to collect samples in fasting. Samples required at least three hours of air drying before returning. DBS samples were transferred to a laboratory for a cardiac profile. This included the assessment of total cholesterol (TC), triglycerides, insulin, hemoglobin glycoset (HBA1C), high-sensitivity protein (HSCRP) and HDL (LDL-C), of Lipl-C (VLDL-C). If the blood volume was inadequate, the markers were prioritized for analysis, starting with HBA1C and HDL-cholesterol.
Predefined gender -related reference areas were used to estimate whether DBS samples were in range. In addition, an electronic research on the collection of data on demographic characteristics (eg age, gender, education, income, relationship status and living arrangements) and health behaviors, including physical activity, nutrition, smoking, sleeping and self-sufficient health. Two research data examined the feasibility of the DBS collection.
The percentage of returned samples was calculated. Chi-Squared and T-tests were carried out to compare the characteristics of the participants among those who returned a sufficient sample and those who did not. In addition, these tests were used to compare the participants who provided sufficient sample for the measurement and the eight cardiovascular markers, regardless of whether they had difficulties in collecting samples.
Findings
DBS collection kits were sent to 506 participants. Of these, 366 returned samples for analysis. Among the kits by post office, 69% of the samples were sufficient to estimate at least one cardiovascular measure, while 46% were sufficient to measure all eight analysts. The difficulties in collecting samples reported by 72% of participants who returned their samples and 38% of those who did not return their samples.
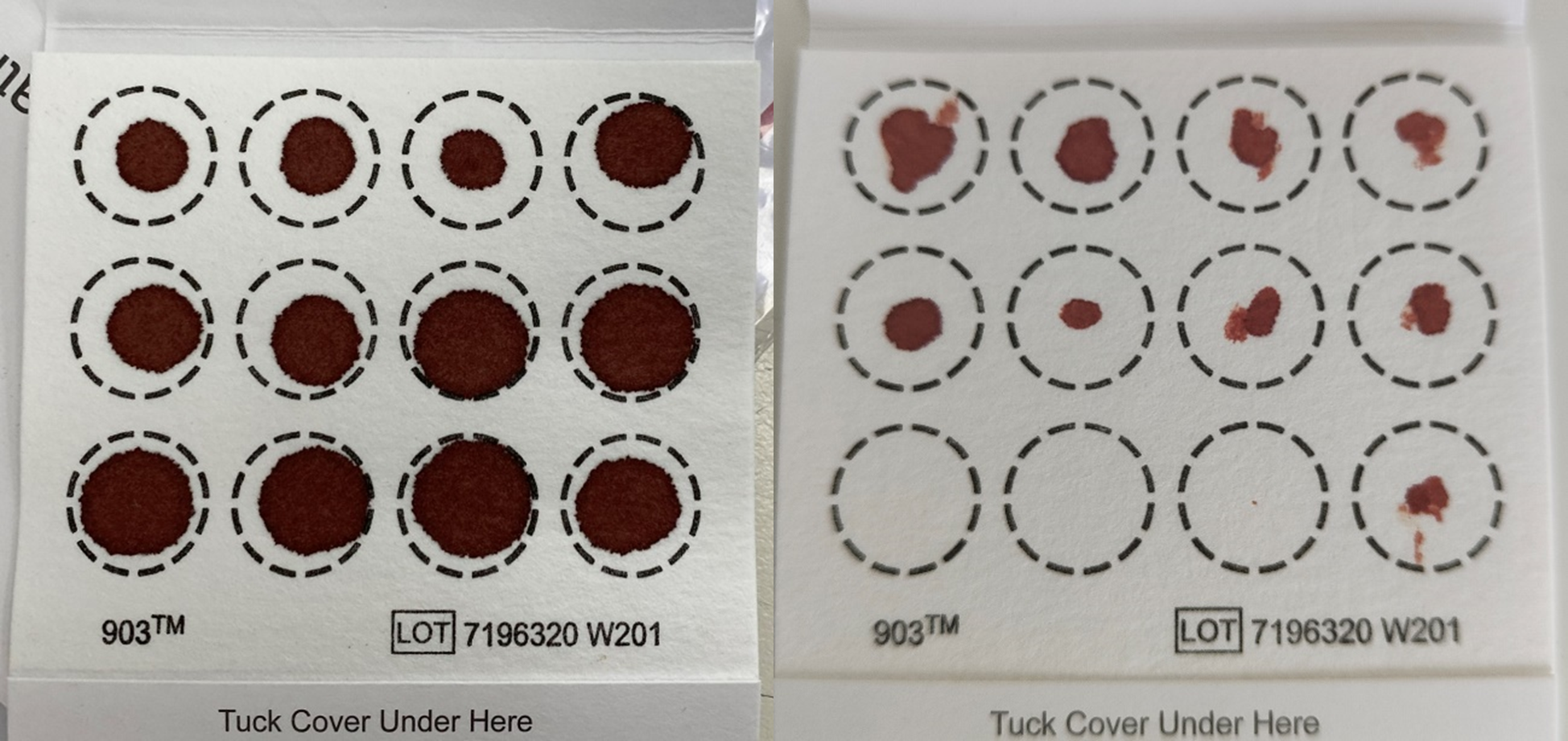
Participating dried examples of blood card collection a) a sample of “good quality” that were sufficient for analysis of all eight cardiac profile indicators and (b) a “poor quality” sample that was sufficient for analysis of only two heart profile profiles.
Specifically, more participants without sampling difficulties provided sufficient sample for all eight meters from those who reported difficulties. The research team noted that the high return rate was probably influenced by the intensive, personalized support they provided. The researchers were preventively contacted 62% of participants who sent kits, following them on average twice each (with some participants receiving up to 12 contacts).
The main challenges were the lack of blood, very few Lancets – that prompted the research team to increase the number provided per kit during the study – escape using Lancets, cold weather and a sense of overwhelmed or scared. People who returned a sufficient sample for all measures were 23.8 years, with an average body mass index (BMI) 26.5 kg/m².
Most participants with a sufficient sample for the measurement of all eight indicators were born in Australia (83%), had a high educational achievement (56%), lived in areas of low socio -economic disadvantages (66%) and covered sleep (78%) and 66%. In addition, 80% reported excellent health, 7% were current smokers and 46% had a history of diabetes or heart disease.
While the authors described many features such as similar, the data revealed a statistically significant response. Participants who did not return their collection cards were much more likely to have lower training and be current smokers than those who returned sample.
The average TC was 187.6 mg/dl, HBA1C was 4.94%, HDL-C was 39.7 mg/dl and LDL-C was 128 mg/dl. The median HSCRP was 0.6 mg/l, insulin was 7.93 one/ml and VLDL-C was 18 mg/dl. About 74% of participants are at risk of at least one cardiovascular index. More men were in danger of HBA1C, insulin and all female lipid markers. In the meantime, there were more females at risk for HSCRP than males.
Conclusions
The study showed moderate success rates for sample adequacy, but also found a statistically significant response bias. Participants who did not return a sufficient sample were more likely to have lower training and being current smokers. The findings suggest that the self-gravited DBS collection is feasible, but emphasizes that its success depends largely on the provision of clear, step-by-step instructions, along with intensive, personalized and preventive support.
Target approaches and practical estimates, such as providing Lancets surpluses, may be needed for different populations to achieve high adequacy. Specifically, the high percentages of the participants were found to be at risk of poor cardiovascular health, stressing the need for control over young adults. However, the authors warn that these findings are not generalized in the wider population. The study sample included a higher percentage of a higher socio -economic position and the authors explicitly state that the results cannot be generalized to reduce socio -economic groups.
Overall, the basic intake of the study is that timely and personalized support, along with clear instructions, is essential to obtain samples of sufficient quality. Specific, practical recommendations for future studies include pilot collection processes and ensuring that kits contain surplus Lancets to tackle the most common difficulty reported by participants.